Home
Public Health
Communicable Disease
Maternal Health
Child Health
Photographs
Documents
Index
You are here
Home
» Dispensary Schedule, p. 2
Dispensary Schedule, p. 2
Document:
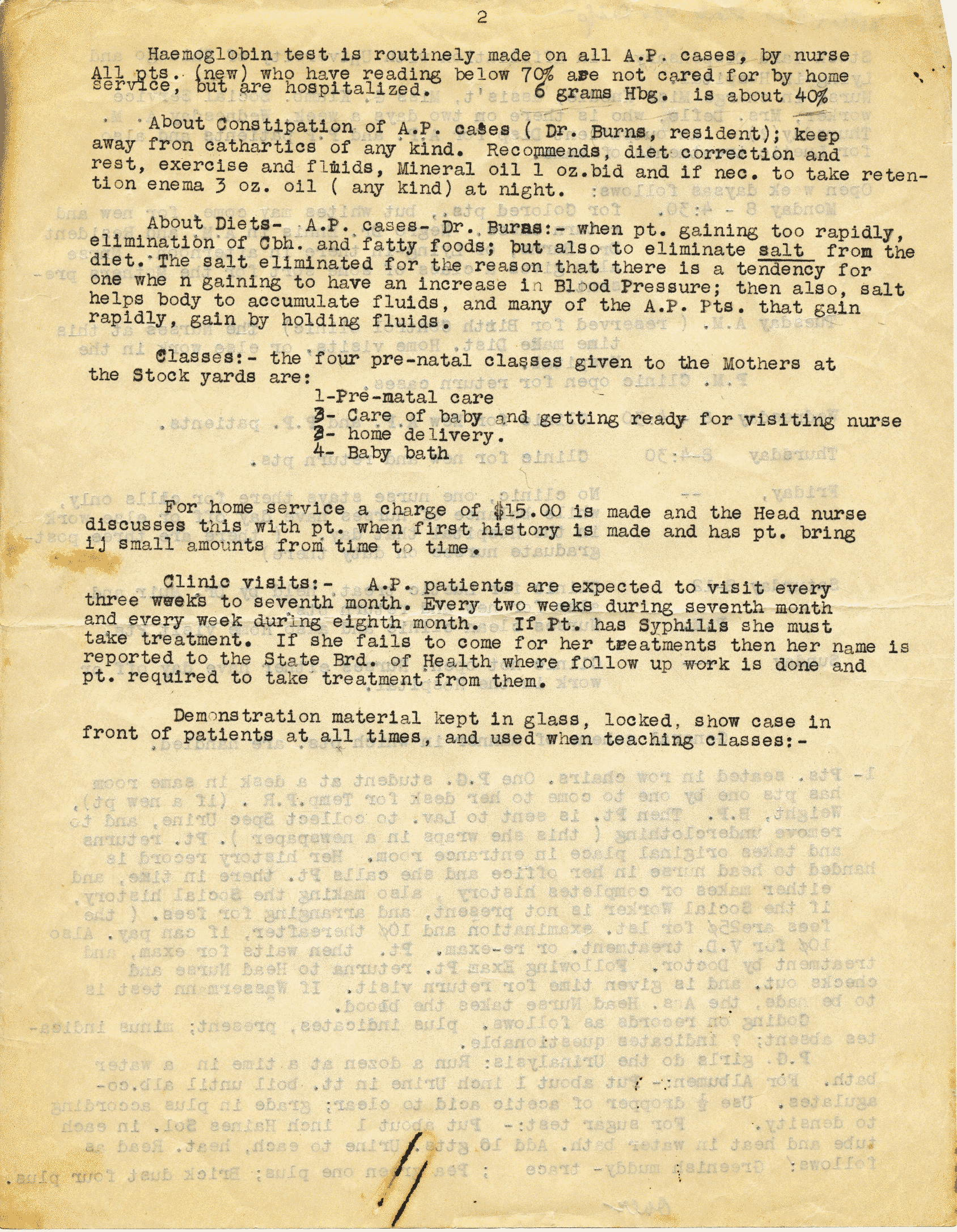
Dispensary Schedule
Number:
p. 2
Person:
Place:
Date: